The Next Pandemic: If We Can’t Respond, We’re Not Prepared
February 28, 2023
This note was also published by the Centre for Disaster Protection here.
Amidst the disastrous impacts of the COVID-19 pandemic, international policy attention on global pandemic prevention, preparedness and response (PPR) has been laudable but has so far proved inadequate. The chance of another deadly pandemic is significant and the potential toll catastrophic, but the current level of global investment in PPR does not yet provide the kind of protection the world needs for effective response.
Estimates of the losses from the COVID pandemic are in the range of $13.8 trillion in lost economic output and between 16.7 million and 27.3 million excess deaths worldwide. The 2014 regional Ebola outbreak in West Africa caused 11,000 deaths and $53 billion in economic losses.
These losses are neither rare nor unusual. We should expect the costs and losses of future infectious disease outbreaks to be high, and an order of magnitude larger than the losses of other severe risks, such as natural disasters or catastrophes (Table 1).
Table 1. Comparison of potential future deaths over a decade by global peril or risk
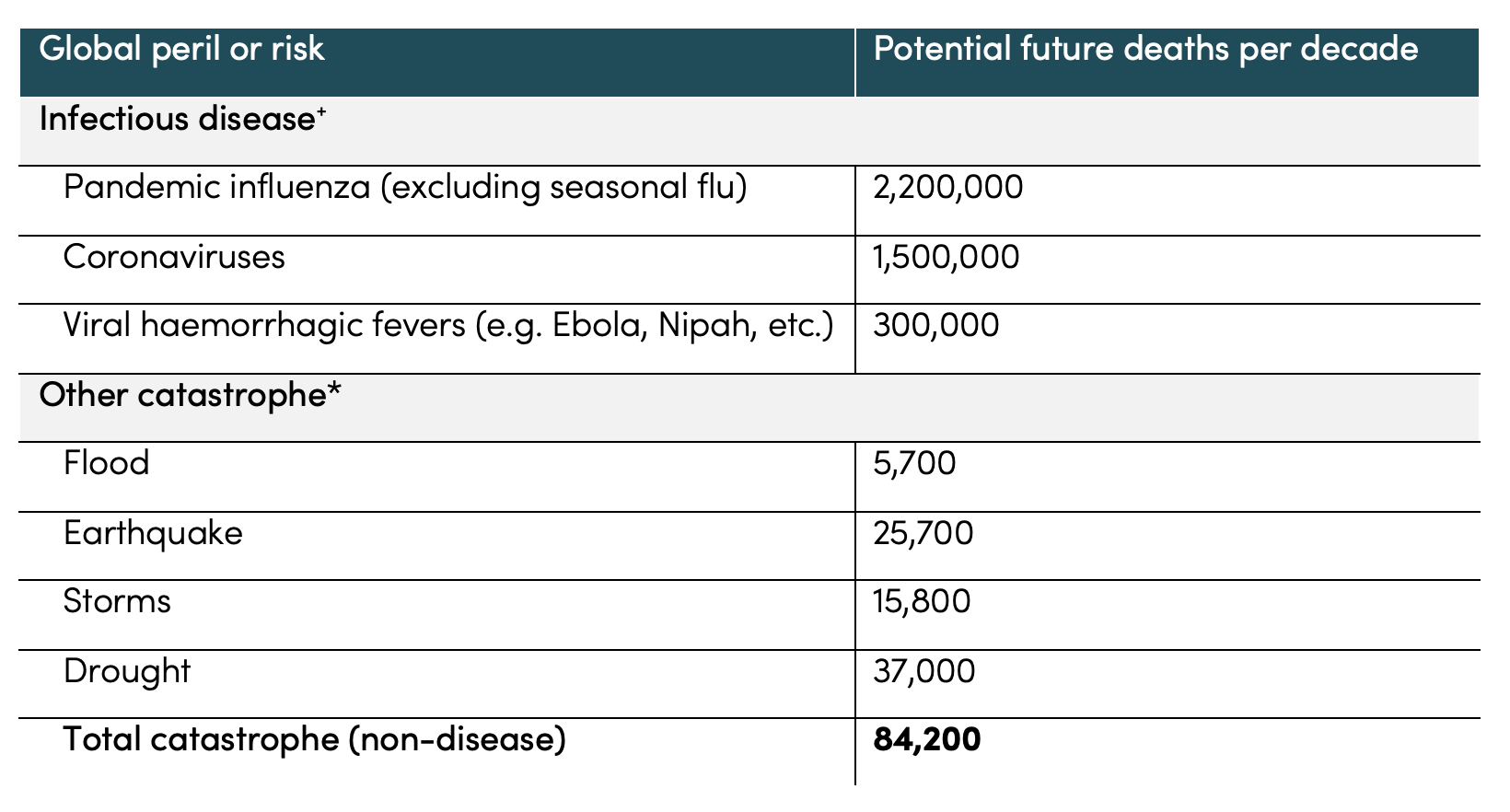
Sources: + Sum of average annual loss (AAL), MetaBiota modelled loss catalogue. * Average decadal loss 1960s-2010s, rounded to nearest hundred calculated using data from OFDA/CRED International Disaster Database—www.emdat.be—Université Catholique de Louvain. Estimates based on models are hard to compare to historical data, and the underlying risk distribution of could be shifting—for example, climate change will make storms more severe and so possibly more deadly. The size of the estimates for infectious disease are based on exceedance probabilities of rare but catastrophic events. The figures suggest the order-of-magnitude costs of disease outbreaks deserve innovation and attention today.
Getting the finance architecture for response right
There are pools of funding available for global humanitarian response, including disease outbreaks. But the financing architecture is not yet the one we need, due to four major concerns: conflicting incentives; fragmented funding; unpredictable funding leading to improvised response; and lack of at-risk advance procurement and pre-positioned manufacturing capacity.
First, conflicting incentives. While the time to report the first cast for high fatality pathogens has improved, declaring an outbreak still carries economic costs and creates an expectation of response. As a result, countries and monitoring organizations trade-off conflicting incentives between declaring an outbreak and waiting for further evidence. In the case of the West African Ebola epidemic of 2014, the outbreak had been correctly identified at a testing facility in Dakar in March 2014 but the World Health Organization (WHO) did not set out a joint response plan until July 2014, and only described the outbreak as a public health emergency of international concern in early August—a delay of six months, which caused unnecessary loss of life and public spending.
Second, fragmented, delayed, and insufficient funding lags disease spread. The current global financing architecture has many smaller-scale, often siloed, financing facilities and instruments. Each facility has different timelines and conditions on access and disbursement, some more opaque than others. This is like trying to pay a bill due yesterday with loose coins and change, it takes months or years to find. The cost of this fragmentation and the absence of clear conditions that would disburse money quickly is that funding lags the rate of transmission instead of leading it.
As a whole, some estimates indicate that the multilateral system collectively mobilized $125 billion to help lower- and middle-income countries tackle COVID between March 2020 and March 2021. But this was piecemeal funding that was mobilized much more slowly than COVID spread and was mainly spent on things like social safety nets and budget support. These are important budget lines that help address the pandemic’s wider impact but largely did not help countries buy or deploy medical countermeasures to slow the disease. And, more broadly, commitments to spend are different from disbursements to countries let alone country spending, indicating a cascade of “global to local” bottlenecks.
Figure 1. Multilateral funding was large but slow compared to COVID’s spread (and mostly not for response)
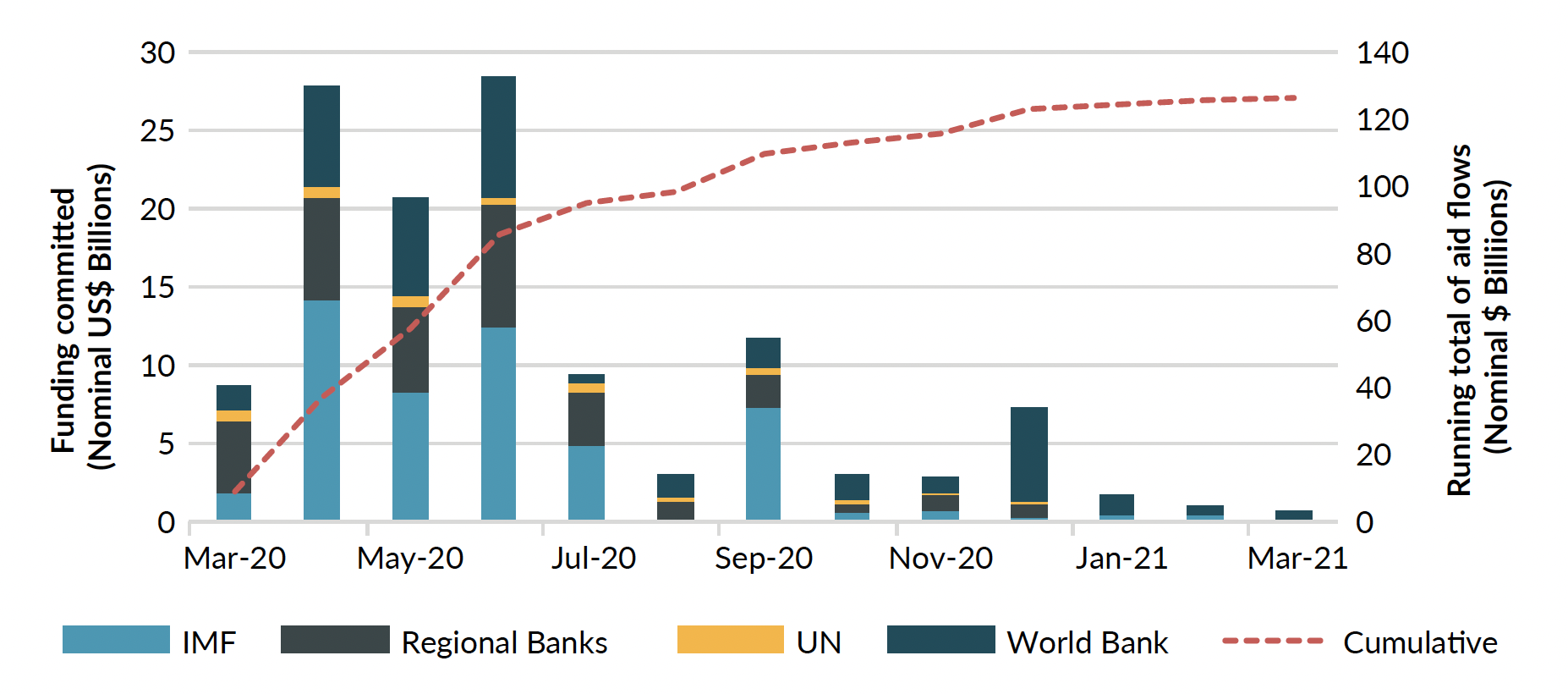
Source: New visualisation of data presented in Yang, Yi, Dillan Patel, R. Hill, and Michèle Plichta. “Funding covid-19 response: tracking global humanitarian and development funding to meet crisis needs.” London: Centre for Disaster Protection.
For funds available to COVAX, the international mechanism for advance purchase of vaccines for lower-income countries, the pace of disbursement was even slower as sufficient funds were not available to pre-commit to purchase vaccines on behalf of low-income countries in ways that would assure early access and supply. Data jointly published by the International Monetary Fund (IMF) and WHO confirm that the bulk of vaccine purchases were secured by rich and relatively rich countries. Vaccine purchases by, and donations to low-income countries were a vanishingly small share of global supply, accounting for just 0.6 percent of total doses between May 2020 and May 2022.
Third, as funding amounts and timing are unpredictable, response happens in an improvised or ad hoc way. Without pre-agreed funding, it is difficult to develop response plans, because planning requires a budget, and building a budget requires a plan. As a result, authorities may not have the staff, stuff, space, systems, and support to rapidly scale-up case detection, provide lab verification, or protect medical workers. This was certainly true for COVID and continues to be true for smaller, localized outbreaks against familiar pathogens.
After the declaration of a recent, new Ebola outbreak in September 2022 in Uganda, for example, health workers denounced the inadequate supply of personal protective equipment and went on strike to protest dangerous working conditions, with a risk of increasing the spread of the disease. And during the same outbreak, fundraising again occurred alongside disease spread with the result that much money likely went unused in the direct response.
Fourth, there is a critical lack of on-call capacity to procure and produce vaccines and other medical countermeasures when outbreaks happen—particularly for emerging pathogens. In the case of COVID, most of the two-year lag between identifying the virus and producing enough vaccine to immunize most of the world was not the time taken to develop the vaccine itself but rather the timing to procure and scale-up manufacturing and production. That lost time from manufacturing and distribution was very costly in terms of lives lost and economic damage.
New economic analysis from Rachel Glennerster and co-authors combines the expected arrival rate of rare-but-deadly outbreaks like coronaviruses with some of their potential costs (like lives lost and economic output, and some long-run social costs like lost education) to estimate the value of producing vaccines at scale, faster. Because the costs of acting late are steep, prepositioning manufacturing capacity and securing financing for production could generate total benefits on the order $400 billion (the net present value of avoided losses).
No preparedness without response
The COVID pandemic generated a wave of interest in PPR. Estimates to date for all-in costs of closing this “preparedness gap” vary (sometimes with opaque costing assumptions), but there is still no plan to reform response financing, the “R” of PPR.
The Pandemic Emergency Financing Facility, or PEF, housed at the World Bank, was an earlier experiment in pre-positioned liquidity and triggers for pandemic response funding. It has since been shut down. The PEF is widely seen as problematic in its design and to date lacks an independent evaluation. Among its issues, the PEF had a disbursement trigger that required evidence of multi-country spread before funds could be released. But by the time cross-border spread occurs, it is often too late to control what happens next. In the case of COVID, this trigger meant delayed disbursement by which time the disease was too widespread to contain, and critically, the mobilized funding was not tied to a pre-agreed plan to control or curb spread.
In September 2022, donors committed $1.4 billion to the Pandemic Fund, managed by the World Bank and involving technical staff from the WHO. The Fund, set up as a financial intermediary fund, concentrates funds for investments in PPR by governments via 13 implementing entities—including multilateral development banks, UN agencies, and organizations such as Gavi, the Vaccine Alliance, and the Global Fund to Fight AIDS, TB and Malaria. Since 136 countries are eligible for support across all elements of PPR set out above, the Pandemic Fund is not placed at present to provide pooled and pre-agreed finance at the scale needed for comprehensive response or pre-positioned production capacity.
There are other health-focused funds that could be scaled up and harmonized. But, for now, they are also relatively small and, in almost all cases, have not integrated clear conditions to release funding—which we call triggers—that pre-position funding against future risks. As an accompanying paper to the Independent Panel for Pandemic Preparedness and Response notes, “[]one month after declaring COVID-19 a Public Health Emergency of International Concern…the WHO’s CFE and another major UN contingency fund – the Central Emergency Response Fund – had allocated a total of just $23.9 million for COVID. Three months later, the UN’s (then) $6.71 billion Global Humanitarian Response Plan was just 5 percent financed; less funding had reached frontline responders.” These and related funding solutions are important but cannot currently guarantee the scale or predictability of funding the world needs for fast response. They are also not designed to enable early-stage research and development.
We need more—and more predictable—finance for response
Disaster risk finance (DRF) is the broad term for a combination of pre-arranged financing (ranging from emergency funds to formal insurance contracts), triggers (the conditions under which the funding is disbursed), and planning (what the money is spent on, when it is triggered). DRF is the financial and process engineering we do today to bank funding we will need tomorrow.
This combination of planning, modelling risk, and pre-positioning finance can inform and potentially revolutionise how we tackle disease outbreaks in four ways:
First, replacing conflicting incentives with aligned incentives. Because the conditions governing the flow of funding are contractually agreed, DRF approaches can help to align incentives between affected countries and monitoring organizations on when to declare an outbreak or enact a response, setting out mutually-agreed conditions to mobilize financing. This will not be easy given the diversity of pandemic risks but should be attempted for those that are well-known such as coronaviruses and influenzas as well as other more regional pandemic threats like Ebola, Marburg, Lassa, and related viruses.
Second, replacing fragmented, opaque, delayed, and insufficient funding with faster, pre-agreed finance. Contracting on risks and triggers dramatically accelerates the delivery of funding, which can then immediately pay for frontline workers, critical equipment, or other inputs to response. When Haiti was struck by a devastating 7.2 magnitude earthquake in August 2021, its sovereign insurance contract paid out $40 million directly to the government in less than two weeks.
Contrast this with outbreaks, when speed and predictability matter because the problem—the number of cases—can grow exponentially. A month after Ebola was detected in Guinea in 2014, for example, estimates called for $5 million to contain it, but after five months of failure to control the spread, the figure was $1 billion. Instead of a large-scale, on-time finance for response, tracking disease deaths and funding mobilized suggests the “tail (of cases) wagged the dog (of funding)”—exactly the opposite of what frontline countries and responders needed then and will need in future outbreaks.
Figure 2. Ebola in 2014: The tail (of cases) wagged the dog (of funding)
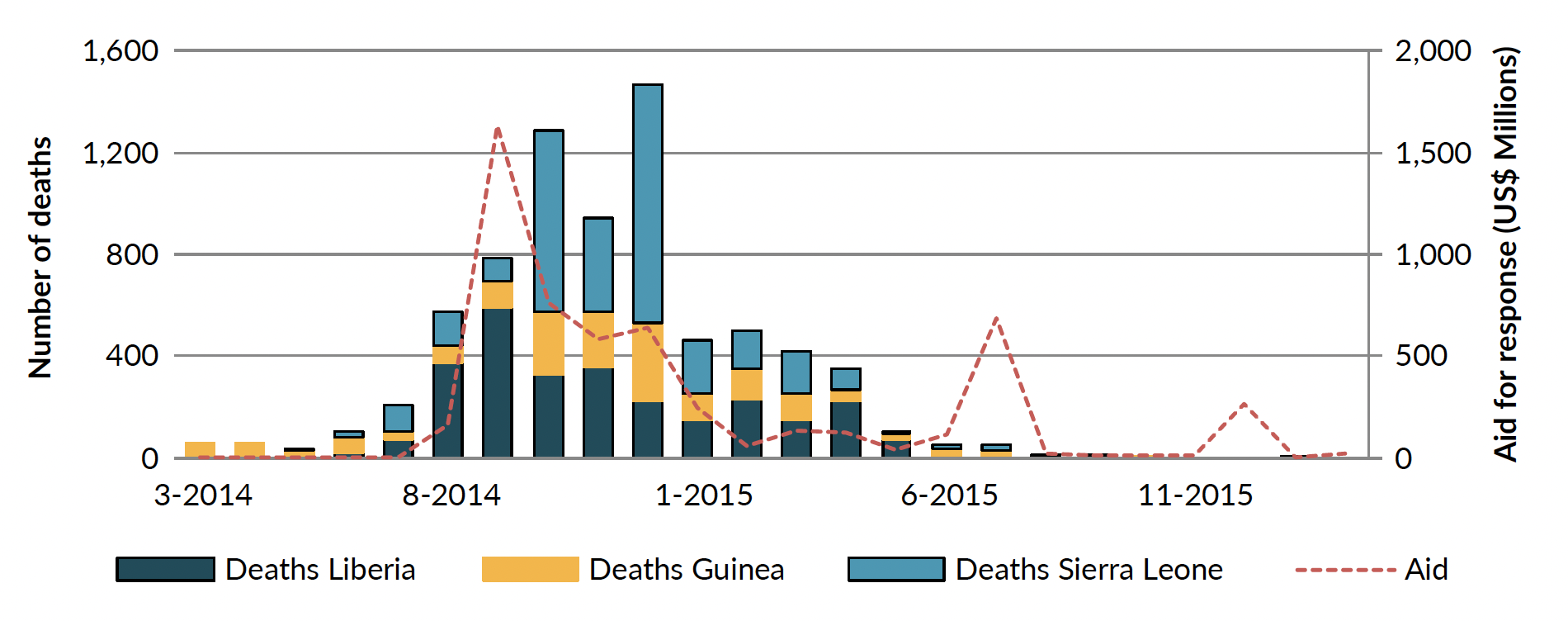
Source: Talbot, Theodore, Stefan Dercon, and Owen Barder. “Payouts for perils: how insurance can radically improve emergency aid.” Center for Global Development. Washington (2017).
Third, replacing improvised or ad hoc planning with pre-agreed plans and advance procurement contracts. Because responding organizations and governments know they will have funding when pre-agreed hazards arrive, they can plan ahead with the knowledge they will have money to enact these response plans. In 2020, the Senegalese government and a group of humanitarian agencies received a joint insurance-style payment of more than $20 million to tackle anticipated food insecurity—the precursor to famine—based on the likelihood of drought picked up from satellite data. The funding enabled a faster, more effective, planned response, helping to avoid worst case scenarios and fundraising during crisis.
Similarly, for relevant pathogens, advance procurement contracts could be developed to signal to R&D organizations and manufacturing firms that there will be real demand, a market, for products in lower-income countries should a public health emergency be declared by national or international authorities. This requires that funders take risks—initial products procured may not be perfectly suited to the disease risk or the country context, or demand may never materialize at the country government level. In these cases, funders must be prepared to absorb losses in the name of a rapid and hopefully effective response in the context of limited budgets. By agreeing to take reasonable risks, funders can capture the high (expected) returns of improved response.
Fourth, replacing production lags with critical capacity to produce future vaccines or other medical countermeasures. The analysis cited earlier finds that the combination of investing $60 billion upfront in vaccine manufacturing capacity today and rapidly mobilizing $5 billion in predictable spending annually would produce enough doses to cover 7 in 10 people globally within six months. Separately, indicative financial modelling show that a lightweight financing structure backed by wealthy countries could be cheap to operate and mobilize on the order of $5 – $10 billion a year for response, including guaranteeing rapid and predictable funding for vaccine production.
What’s next?
The policy discussions about PPR are noteworthy. But the global public sector is underinvesting in pandemic response. This creates the illusion of safety without the finance or planning in place to provide it.
By applying disaster risk finance tools and instruments to containing outbreaks, countries can have faster liquidity, nimbler coordination, and adequate scale of ready financing. We cannot delay planning for response financing when the next pandemic hits, by which time it would be too late. We need to plan for response financing today.
Over the coming year, the Centre for Disaster Protection and the Center for Global Development will look to collaborate to understand the lessons of disaster risk financing for pandemic or epidemic response financing, review the ways that countries themselves include pandemic risks in national preparedness plans and budgets, and develop policy options to put contingent response financing in place internationally ahead of the next global or regional pandemic risk.
Preparedness will help reduce the need for response, but it does not eliminate it—the global community must take the next step.
Learn more